
I Just Tore my ACL – Now What?

A huge thank you to Zack Vint for putting together this blog - enjoy!
Picture this – you’re running down the field playing a game of soccer with your friends. You’re chasing the ball, but you have to make a sudden hard change in direction and then…
“POP!”
You find yourself on the ground holding your knee in intense pain, and immediately you can tell something feels off. Your friends quickly take you to the emergency room, and after a long wait the attending doctor informs you that you have ruptured your ACL and that you will need surgery. You are quickly sent on your way with a referral to an orthopedic surgeon, left with countless questions:
- What did I hurt?
- How long is my recovery going to take?
- Will my knee ever be the same?
- Do I need surgery?
- What even is an ACL?
Unfortunately, this is the position so many people find themselves in. In this blog post we aim to help answer some of these questions and provide a bit of guidance through the murky waters of ACL rehab!
What is an ACL?
Often you can’t get through an episode of Sports Centre without hearing about an ACL injury, so it is not surprising that most people are usually familiar with the term. Despite this, I have found that most people actually don’t know what the ACL is or what it even does.
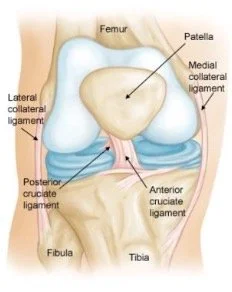
Picture courtesy of orthoinfo.aaos.org
The term ACL is an abbreviation for a ligament in our knee known as the Anterior Cruciate Ligament. As pictured in the diagram above, it is the closest of the two ligaments that cross in the centre of the knee, hence the name cruciate. Its role is to help provide stability to the knee and resist rotational forces. In fact, one of the key indications of ACL involvement are injuries that stress the function of this ligament like a rapid change of direction with a planted foot. If this is combined with feeling of a “Pop” and rapid swelling of the knee, we can be fairly certain you damaged your ACL.
What Options are Available?
Classically there are three management strategies following ACL rupture:
1. Rehabilitation: Otherwise known as conservative management, rehabilitation involves regular physical therapy and structured exercise. You can expect treatments to eliminate swelling, mobility drills to regain movement, and ultimately resistance training to help improve strength and confidence in your knee.
2. Early surgical reconstruction followed by rehabilitation: Typically, early surgery is considered any operation within the first month of ACL injury. The surgeon will take tissue from elsewhere in your body, usually from your hamstring or quadriceps tendon, and use it to construct a graft and make a new “ACL” for your knee. What is important to highlight is that surgery is no quick fix – recovery and rehabilitation after the operation can be grueling and even more intensive than rehabilitation alone.
3. “Wait and See” - Preoperative rehabilitation, followed by delayed surgery, and post operative rehabilitation: This is the most common approach for ACL management in Canada, as we are unable to access surgery early due to long wait lists. Likewise, if you are not having a lot of success with rehabilitation alone, ACL reconstruction can always remain an option.
Will My Knee Ever be the Same?
While we want to be optimistic about recovery, it is important to first set realistic expectations. For most people, their knee will never quite feel the same; a common complaint being a lack of trust in the knee. In fact, along with fear of reinjury, lack of trust is the most common reason for why people don’t return to sport, or their previous levels of activity. These sentiments make sense when we consider that following an ACL rupture, you are at a much greater risk for a future knee injury and developing knee osteoarthritis at some point in your life.
Ultimately, an important step in recovery is acknowledging that in many ways, the knee joint has undergone a permanent change. Despite this, there are steps that we can take to set you up for success. First, it is important to realize that there is an elevated risk of reinjury with returning to sports and activities that involve cutting, pivoting, and contact (soccer, football, hockey, etc.). While the most efficient way to minimize this risk is through avoiding and modifying these activities, for many people this is not an option. If you are someone who aspires to participate in all the same activities, the best approach is to respect the time it takes for our body to heal and follow through on a complete gradual return to activity protocol. More specifically, you can expect a 9 – 12 month recovery following ACL reconstruction, or a slightly shorter time-frame if you decide to pursue rehabilitation alone. Regardless of the management approach, the biggest priority is helping you return to the things your love while maintaining a physically active lifestyle; all together, helping to prevent the development of osteoarthritis.

Which Option Should I Pursue?
We used to believe that to minimize future injury and maximize potential knee function, it was necessary to undergo an ACL reconstruction. We now understand that this may not be the case.
When we look at what the research tells us, there appears to be very similar outcomes between surgical and non-surgical interventions. More specifically, when we look at knee re-injury rates (including, other ligament, meniscus, and cartilage injuries) we see that you have an equal chance of re injuring the knee regardless of management approach. Likewise, it doesn’t appear that opting out of surgery increases your risk for developing osteoarthritis; in fact, early surgery may even elevate this risk.
A common myth is that you need to undergo ACL reconstruction to be able to return to pivoting sports. Numerous studies contradict this belief, demonstrating no difference in physical activity levels between those managed conservatively or surgically. Similarly, rehabilitation alone shows the same rate of return to sport as surgery. All together, we see similar levels of knee function, activity level, quality of life, and functional stability regardless of treatment approach. So, considering all of this – why would we ever perform surgery?
Current recommendations suggest that the first line of management for ACL injury should involve the “Wait and see” approach as outlined in Option 3 in the previous section. Specifically, it is suggested to trial rehabilitation alone and delay the decision for surgery until the knee is “Quiet” (mobility, strength, and swelling returned close to preinjury levels). Surgery is only indicated, if you feel as though you have not returned to your desired level of function and activity. Despite many finding success with rehabilitation, this is the unfortunate reality for some people.
Can the ACL Heal?
If you were to ask this question 20 years ago, the answer would be a resounding NO! Interestingly, as there has been further investigation into ACL recovery over the past couple of decades, there have been cases where the ACL has shown signs of healing on MRI.
Recently in a more rigorous study, researchers demonstrated ACL healing in 1/3 of their participants who underwent rehabilitation only. What’s even more interesting, is that these individuals had better outcomes and were less likely to request surgery compared to those who did not have any signs of healing. This suggests a potential explanation for why different people experience varying success with conservative management.
While we are now confident that the ACL can heal on its own, we have still yet to answer why it heals only in certain cases. One thought is that by reducing the distance between the two torn ends, we may be able to facilitate healing. A newly developed bracing protocol attempted to answer this question by immobilizing the knee in a bent position for 4 weeks. Remarkably, they reported that of the 80 people managed with this method, 90% had signs of healing on MRI. Although promising, more information is needed before we can confidently make any recommendations about this novel approach. Regardless, it is exciting that this maybe the new standard of care for ACL management in the future.
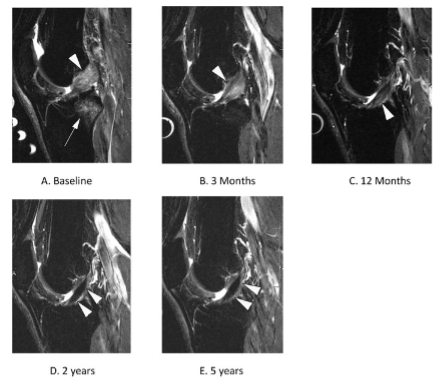
ACL healing demonstrated on MRI: Taken from Filbay et al., 2023
Concluding Thoughts
ACL ruptures are complex injuries that require physical, psychological, and emotional support. It is not uncommon to feel lost and confused following the injury, especially with the overwhelming amount of misinformation surrounding ACL rupture. It is important to realize while your knee may never feel the same, there are a number of treatment options available to help you regain function in your knee. Overall, our body is incredibly resilient and capable of demonstrating remarkable feats of healing. With appropriate injury management, patience, and progressive rehabilitation, I am confident that even with an ACL injury you can always get back to doing the things you love.
References
Ex los angeles rams WR Odell Beckham played 'without ACL' during Super ... (n.d.). Retrieved May 2, 2023, from https://www.si.com/nfl/rams/news/los-angeles-rams-wide-receiver-odell-beckham-acl-injury-news-baltimore-ravens-contract-signing
Filbay, S. R., Dowsett, M., Jomaa, M. C., Rooney, J., Sabharwal, R., Lucas, P., Van Den Heever, A., Kazaglis, J., Merlino, J., Moran, M., Allwright, M., Kuah, D., Durie, R., Roger, G., Cross, M., & Cross, T. (2023). A novel non-surgical bracing protocol may facilitate healing of anterior cruciate ligament rupture and improve clinical outcomes. Osteoarthritis and Cartilage, 31. https://doi.org/10.1016/j.joca.2023.01.178
Filbay, S. R., & Grindem, H. (2019). Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture. Best practice & research. Clinical rheumatology, 33(1), 33–47. https://doi.org/10.1016/j.berh.2019.01.018
Filbay, S. R., Roemer, F. W., Lohmander, L. S., Turkiewicz, A., Roos, E. M., Frobell, R., & Englund, M. (2023). Evidence of ACL healing on MRI following ACL rupture treated with rehabilitation alone may be associated with better patient-reported outcomes: a secondary analysis from the KANON trial. British journal of sports medicine, 57(2), 91–98. https://doi.org/10.1136/bjsports-2022-105473
Frobell, R. B., Roos, E. M., Roos, H. P., Ranstam, J., & Lohmander, L. S. (2010). A randomized trial of treatment for acute anterior cruciate ligament tears. The New England journal of medicine, 363(4), 331–342. https://doi.org/10.1056/NEJMoa0907797
Webster, K. E., & Hewett, T. E. (2022). Anterior Cruciate Ligament Injury and Knee Osteoarthritis: An Umbrella Systematic Review and Meta-analysis. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine, 32(2), 145–152. https://doi.org/10.1097/JSM.0000000000000894
Whittaker, J. L., Culvenor, A. G., Juhl, C. B., Berg, B., Bricca, A., Filbay, S. R., Holm, P., Macri, E., Urhausen, A. P., Ardern, C. L., Bruder, A. M., Bullock, G. S., Ezzat, A. M., Girdwood, M., Haberfield, M., Hughes, M., Ingelsrud, L. H., Khan, K. M., Le, C. Y., Losciale, J. M., … Crossley, K. M. (2022). OPTIKNEE 2022: consensus recommendations to optimise knee health after traumatic knee injury to prevent osteoarthritis. British journal of sports medicine, 56(24), 1393–1405. https://doi.org/10.1136/bjsports-2022-106299
Whittaker, J. L., Losciale, J. M., Juhl, C. B., Thorlund, J. B., Lundberg, M., Truong, L. K., Miciak, M., van Meer, B. L., Culvenor, A. G., Crossley, K. M., Roos, E. M., Lohmander, S., & van Middelkoop, M. (2022). Risk factors for knee osteoarthritis after traumatic knee injury: a systematic review and meta-analysis of randomised controlled trials and cohort studies for the OPTIKNEE Consensus. British journal of sports medicine, 56(24), 1406–1421. https://doi.org/10.1136/bjsports-2022-105496